Fill Out Your DD 2870 Template
Fill Out Your DD 2870 Template
Accessing medical records or designating someone to access them on your behalf is a crucial step in managing healthcare efficiently. Whether it's for a personal health issue, for insurance claims, or for facilitating care from different healthcare providers, having the right documentation is key. This is where the Department of Defense (DoD) form 2870, also known as the Authorization for Disclosure of Medical or Dental Information, comes into play. It serves as a vital tool for individuals associated with the military—whether active duty members, veterans, or dependents—to authorize the release of their medical or dental information to specified parties. This form not only ensures that personal health information is handled securely but also complies with privacy regulations, safeguarding sensitive information. With this document, individuals can specify what information can be disclosed, to whom, and for what purpose, ensuring their medical data is shared according to their preferences and needs.
Prescribed by: DoDM 6025.18 |
CONTROLLED when filled |
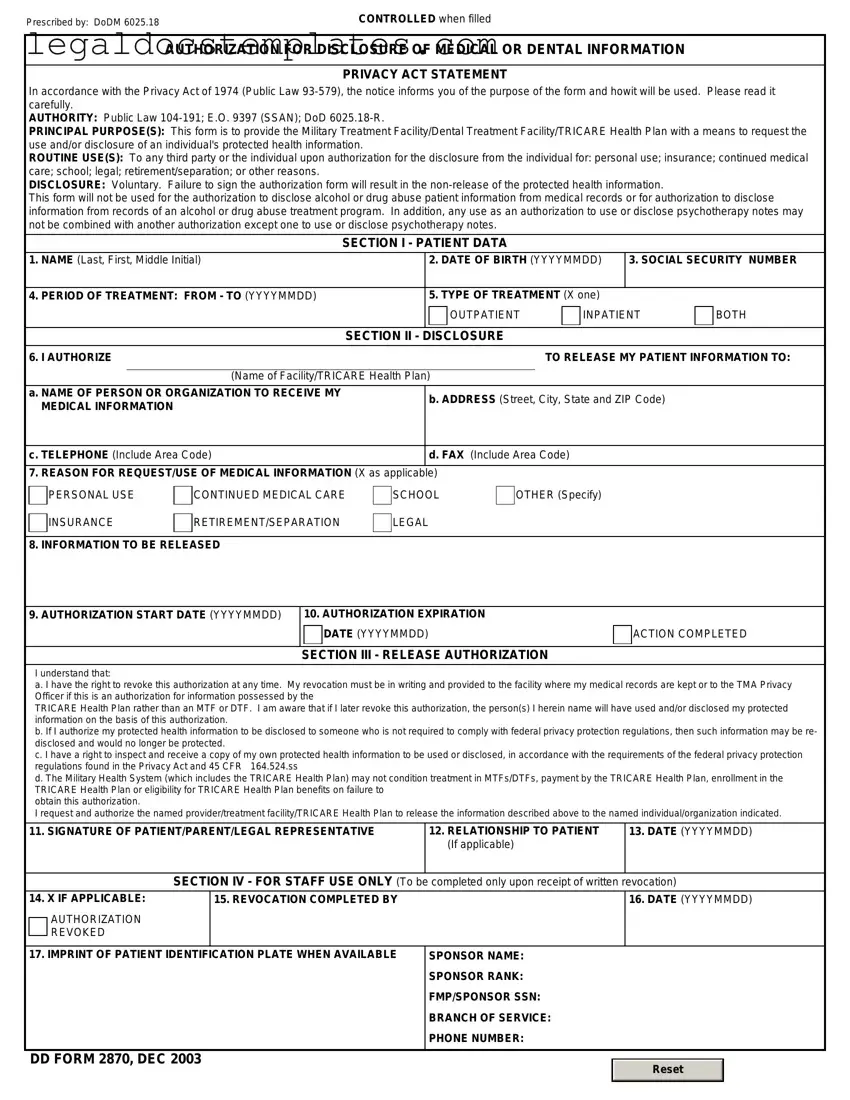
AUTHORIZATION FOR DISCLOSURE OF MEDICAL OR DENTAL INFORMATION
PRIVACY ACT STATEMENT
In accordance with the Privacy Act of 1974 (Public Law
AUTHORITY: Public Law
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/or disclosure of an individual's protected health information.
ROUTINE USE(S): To any third party or the individual upon authorization for the disclosure from the individual for: personal use; insurance; continued medical care; school; legal; retirement/separation; or other reasons.
DISCLOSURE: Voluntary. Failure to sign the authorization form will result in the
This form will not be used for the authorization to disclose alcohol or drug abuse patient information from medical records or for authorization to disclose information from records of an alcohol or drug abuse treatment program. In addition, any use as an authorization to use or disclose psychotherapy notes may not be combined with another authorization except one to use or disclose psychotherapy notes.
SECTION I - PATIENT DATA
1. NAME (Last, First, Middle Initial) |
|
2. DATE OF BIRTH (YYYYMMDD) |
3. SOCIAL SECURITY NUMBER |
|||
|
|
|
|
|
|
|
4. PERIOD OF TREATMENT: FROM - TO (YYYYMMDD) |
|
5. TYPE OF TREATMENT (X one) |
|
|
||
|
|
|
OUTPATIENT |
INPATIENT |
BOTH |
|
|
|
|
|
|
|
|
|
|
SECTION II - |
DISCLOSURE |
|
|
|
6. I AUTHORIZE |
|
|
TO RELEASE MY PATIENT INFORMATION TO: |
|||
|
|
|
|
|
||
|
(Name of Facility/TRICARE Health Plan) |
|
|
|
||
a. NAME OF PERSON OR ORGANIZATION TO RECEIVE MY |
|
b. ADDRESS (Street, City, State and ZIP Code) |
|
|||
MEDICAL INFORMATION |
|
|
||||
|
|
|
|
|
||
|
|
|
|
|
||
c. TELEPHONE (Include Area Code) |
|
d. FAX (Include Area Code) |
|
|
||
|
|
|
|
|
||
7. REASON FOR REQUEST/USE OF MEDICAL INFORMATION (X as applicable) |
|
|
|
|
||
PERSONAL USE
INSURANCE
CONTINUED MEDICAL CARE
RETIREMENT/SEPARATION
SCHOOL
LEGAL
OTHER (Specify)
8. INFORMATION TO BE RELEASED
9. AUTHORIZATION START DATE (YYYYMMDD)
10. AUTHORIZATION EXPIRATION
DATE (YYYYMMDD)
SECTION III - RELEASE AUTHORIZATION
ACTION COMPLETED
I understand that:
a. I have the right to revoke this authorization at any time. My revocation must be in writing and provided to the facility where my medical records are kept or to the TMA Privacy Officer if this is an authorization for information possessed by the
TRICARE Health Plan rather than an MTF or DTF. I am aware that if I later revoke this authorization, the person(s) I herein name will have used and/or disclosed my protected information on the basis of this authorization.
b. If I authorize my protected health information to be disclosed to someone who is not required to comply with federal privacy protection regulations, then such information may be re- disclosed and would no longer be protected.
c. I have a right to inspect and receive a copy of my own protected health information to be used or disclosed, in accordance with the requirements of the federal privacy protection regulations found in the Privacy Act and 45 CFR 164.524.ss
d. The Military Health System (which includes the TRICARE Health Plan) may not condition treatment in MTFs/DTFs, payment by the TRICARE Health Plan, enrollment in the TRICARE Health Plan or eligibility for TRICARE Health Plan benefits on failure to
obtain this authorization.
I request and authorize the named provider/treatment facility/TRICARE Health Plan to release the information described above to the named individual/organization indicated.
11. SIGNATURE OF PATIENT/PARENT/LEGAL REPRESENTATIVE |
12. RELATIONSHIP TO PATIENT |
13. DATE (YYYYMMDD) |
|
(If applicable) |
|
|
|
|
SECTION IV - FOR STAFF USE ONLY (To be |
completed only upon receipt of written revocation) |
|
14. X IF APPLICABLE:
AUTHORIZATION REVOKED
15. REVOCATION COMPLETED BY
16.DATE (YYYYMMDD)
17. IMPRINT OF PATIENT IDENTIFICATION PLATE WHEN AVAILABLE |
SPONSOR NAME: |
||
|
SPONSOR RANK: |
||
|
FMP/SPONSOR SSN: |
||
|
BRANCH OF SERVICE: |
||
|
PHONE NUMBER: |
||
|
|
|
|
DD FORM 2870, DEC 2003 |
|
|
|
|
Reset |
|
|
|
|
|
|
|
|
|
|
| Fact Name | Description |
|---|---|
| Form Title | DD Form 2870, Authorization for Disclosure of Medical or Dental Information |
| Purpose | Used to authorize disclosure of medical or dental information by military health care providers to designated parties. |
| Users | Primarily utilized by service members, veterans, and their families. |
| Information Required | Includes personal identification details, information on the health records requested, and the name of the individual or entity authorized to receive the information. |
| Privacy Act Statement | Contains a notice regarding the Privacy Act of 1974, explaining the purpose of the form and the usage of the requested information. |
| Consent Validity | The authorization remains valid for a specified duration, generally not exceeding one year, unless otherwise revoked. |
| Governing Regulations | Governed by the Health Insurance Portability and Accountability Act (HIPAA) and the Privacy Act of 1974. |
Filling out the DD 2870 form is a critical step for requesting the release of medical or dental records. This process, while straightforward, requires attention to detail to ensure that all the necessary information is accurately provided. The steps outlined below are designed to guide individuals through the process smoothly and efficiently. By following these instructions, you can complete the form correctly and expedite your request.
Once completed, review the form to ensure all the information provided is correct and complete. Submitting an accurately filled out form is crucial for a smooth and quick process. If you have any questions or require assistance, don't hesitate to contact the appropriate office or department handling the DD 2870 form submission.
The DD 2870 form, also known as Authorization for Disclosure of Medical or Dental Information, is used to request the release of medical or dental records. It grants permission to healthcare providers to share an individual's health information with specified parties.
This form can be submitted by the individual whose records are being requested, or their legal representative. In the case of minors, a parent or legal guardian must submit the form.
Completing the DD 2870 form requires several pieces of information, including:
The completed form should be submitted directly to the healthcare provider holding the records. It's recommended to confirm the preferred method of submission, such as by mail, fax, or hand delivery, with the provider.
Fees may vary depending on the healthcare provider's policies and the amount of records requested. Contact the provider directly to inquire about any associated costs.
Processing times can vary widely based on the healthcare provider's policies, the volume of requests, and the type of records requested. Generally, it can take from a few days to several weeks.
If your request is denied, first review the denial reason provided by the healthcare provider. You may need to submit additional information or clarify your request. For further assistance, consider consulting with a legal advisor.
Yes, the DD 2870 form allows you to specify particular types of information you want released. Clearly state these preferences in the designated section of the form.
Yes, you can revoke the authorization at any time. To do so, notify the healthcare provider in writing, specifying the date the revocation is to take effect.
Copies of the DD 2870 form can be obtained from military healthcare facilities, or you can download the form from the official website of the Department of Defense or other related government websites.
Filling out the DD 2870 form, or Authorization for Disclosure of Medical or Dental Information, is an essential step in managing one’s healthcare records within the military health system. However, errors can occur during this process, affecting the timeliness and privacy of your medical information. Recognizing and avoiding these mistakes is crucial for ensuring your healthcare management is both efficient and secure.
One common mistake is not specifying the type of information to be disclosed. The DD 2870 form requires individuals to clearly identify whether they want medical records, dental records, or both. Without this specification, the processing of the request can be delayed significantly. It's important to check the appropriate box or provide detailed information in the space provided to ensure the request is processed without unnecessary delays.
Inadequate identification of the recipient is another frequent error. The form asks for detailed information about who will receive the disclosed information. This includes the recipient's full name, address, and possibly their relationship to the requester. Failing to provide complete and accurate information can lead to the mishandling of sensitive medical data, breaching privacy, and potentially causing personal information to be sent to the wrong party.
Another mistake involves neglecting to specify the purpose of the disclosure. Whether the information is being disclosed for insurance purposes, ongoing medical care, or legal reasons, it must be stated clearly. This clarity helps ensure that only the necessary information is shared, safeguarding the patient’s privacy and adherence to regulations concerning medical information disclosure.
A critical yet often overlooked error is not giving a proper expiration date for the authorization. If the form is submitted without specifying when the authorization ends, it might result in the authorization being either too short, limiting its usefulness, or indefinitely long, which could pose privacy concerns. It is advised to carefully consider and clearly indicate the timeframe for which the disclosure is permitted.
Failure to sign and date the form represents a pivotal mistake. The DD 2870 form requires the signature of the individual authorizing the release of their information, or their legal representative if the individual is not capable of signing themselves. Without this signature, the request is not valid, and no action can be taken to release the requested information. This often results in delays and necessitates the completion of a new form.
Last but not least, overlooking the need to check with the specific medical or dental facility for additional requirements can cause delays. While the DD 2870 form provides a standardized means of requesting information, individual facilities may have their own protocols or additional forms that need to be completed. Failing to comply with these specific requirements can lead to significant processing delays.
In summary, while filling out the DD 2870 form might seem straightforward, paying attention to these common mistakes can greatly influence the efficient and secure processing of your medical information disclosure request. By meticulously avoiding these errors, you ensure your healthcare management is conducted smoothly and your private information is handled with the utmost care.
When individuals engage with the DD 2870 form, a document that authorizes the disclosure of medical or dental information, they often find themselves navigating through a series of additional forms and documents. These materials, crucial for various procedures related to healthcare, medical benefits, and personal records management within military contexts, serve distinct yet interconnected purposes. Understanding these forms can significantly streamline the process of managing one’s healthcare information or that of a loved one.
Each document above supports the comprehensive management of health and medical services for individuals within the military and veteran communities. By familiarizing themselves with these forms, service members, veterans, and their families can better navigate the complexities of healthcare access and privacy, ensuring they receive the benefits and care they deserve. It’s a testament to the interconnected nature of healthcare administration and the importance of informed consent and records access in maintaining transparency and trust between individuals and healthcare providers.
The DD 2870 form, also known as the Authorization for Disclosure of Medical or Dental Information, allows military personnel and their families to authorize the release of their medical records. This form is quite similar to the HIPAA Release Form used widely across the civilian healthcare system. The HIPAA Release Form also provides consent for the disclosure of personal health information, ensuring that the process adheres to the Health Insurance Portability and Accountability Act (HIPAA) guidelines. Both forms serve a critical role in protecting patients' privacy while allowing necessary medical information sharing.
Another document similar to the DD 2870 is the General Authorization for Release of Medical Records form often found in civilian hospitals and clinics. This form, like the DD 2870, is used to grant permission to healthcare providers to exchange pertinent medical information with other entities, such as insurance companies or other healthcare providers, to support the patient's treatment, payment activities, or healthcare operations.
The VA Form 10-5345, Request for and Authorization to Release Medical Records or Health Information, shares similarities with the DD 2870. Used by the Department of Veterans Affairs, this form allows veterans to authorize the disclosure of their health information for various purposes. Both forms respect the privacy of the individual's health information while facilitating the sharing of data when authorized by the patient.
The Consent to Release Financial Information form, while not specific to healthcare, shares a conceptual function with the DD 2870. It permits the sharing of an individual’s financial records with authorized parties. Like the DD 2870, which deals with medical or dental records, this form underscores the importance of confidentiality and the need for explicit permission before any personal data is disclosed.
Form SSA-827, Authorization to Disclose Information to the Social Security Administration, is another document that parallels the DD 2870. This form grants the SSA permission to obtain medical, educational, and other information necessary to evaluate a claim for benefits. Both the SSA-827 and the DD 2870 are crucial in ensuring that sensitive information is shared legally and ethically to aid in benefit determination and healthcare.
The Medical Information Release Form (HIPAA), often specific to individual healthcare providers, similarly requires a patient’s consent to release their health information. This form typically caters to the guidelines set forth by HIPAA, emphasizing privacy and the proper handling of medical records, echoing the core purposes of the DD 2870.
The Authorization for Release of Psychological Records is a specialized form specific to mental health services. It allows for the disclosure of sensitive psychological records under the patient's consent. While it’s more specific in scope compared to the DD 2870, both documents ensure that highly confidential information is protected and only released according to the patient’s wishes.
The Educational Records Release Form, used within educational institutions, authorizes the disclosure of a student's academic records. Though its primary focus is not health-related, the consent process mirrors that of the DD 2870, emphasizing individual rights and the controlled sharing of personal information.
Lastly, the Power of Attorney (POA) for Healthcare is a legal document appointing someone to make healthcare decisions on another’s behalf. It intersects with the intent of the DD 2870 insofar as it deals with personal health information, albeit from the standpoint of decision-making authority rather than direct information sharing. Both documents are important in managing health information and ensuring decisions are made in the best interest of the individual.
Each of these documents, while varying in focus and application, shares the common theme of safeguarding personal information. Whether it's health records, financial information, or educational data, the principle of informed consent is central. The DD 2870 and its counterparts are vital tools in managing privacy and consent in a complex information-sharing environment.
Filling out the DD 2870 form, also known as the Authorization for Disclosure of Medical or Dental Information, demands attention to detail and a thorough understanding of what is both required and cautioned against. The process not only involves handling sensitive information but also ensuring that the privacy and rights of the individual are preserved. Below is a compiled list of dos and don'ts to guide you through the completion of the DD 2870 form.
Do:The DD 2870 form, also known as the Authorization for Disclosure of Medical or Dental Information, is surrounded by misconceptions. These misunderstandings can complicate the process of sharing necessary health information. Here are ten common misconceptions debunked:
Only military personnel can use the DD 2870. In reality, the form can be used by both military members and their dependents, allowing a broad range of individuals to authorize the disclosure of their health information.
It allows for the release of information to anyone. The form only permits the disclosure of medical or dental information to entities or individuals specified by the person signing the form. This means the release is controlled and not open-ended.
The DD 2870 covers all types of information release. It is specifically designed for medical or dental information, not other types of personal data. Misunderstanding the scope can result in misusing the form.
Signing the form gives permanent consent. Consent given through the DD 2870 is not indefinite. The form includes a section for specifying the duration of the authorization, ensuring time-bound consent.
The process is complicated. The DD 2870 form is straightforward. It is structured to guide individuals through specifying the type of information to be released, to whom, and for how long.
It's only applicable in the United States. While primarily used within the U.S. military health system, the authorization can facilitate the transfer of needed medical information to entities outside the U.S., given the recipient is specified in the form.
The form can be submitted electronically by anyone. Electronic submissions may require verification of the requester's identity and their authority to request such information, which can restrict who can submit the form electronically.
Any medical professional can initiate this request. The DD 2870 form is initiated by the patient or their legal representative, rather than by medical professionals seeking information.
There's no need to renew authorization for continuous care. For ongoing information sharing, especially for chronic conditions or long-term treatments, it might be necessary to renew the authorization once the specified duration expires.
Using the DD 2870 infringes on patient privacy. Patient privacy is a critical concern, and the use of the DD 2870 form adheres to stringent privacy laws, ensuring that information is shared securely and only according to the patient’s explicit wishes.
Understanding these misconceptions helps in correctly using the DD 2870 form, ensuring that the authorization for the disclosure of medical or dental information is smooth and secure. Remember, it's always wise to consult with a healthcare professional or legal advisor if there are any questions or concerns about using the form.
The DD 2870 form, or Authorization for Disclosure of Medical or Dental Information, is an important document used within the Department of Defense. It facilitates the sharing of medical or dental information between authorized individuals and organizations. Understanding how to properly fill out and use this form is crucial for ensuring that sensitive information is handled correctly. Below are eight key takeaways:
How to Change Your Address for Mail - Regular updates to your address using the PS 3575 form can help maintain accurate records and smooth delivery of postal services.
Sample Profit and Loss Statement - By analyzing this form, businesses can make informed decisions about pricing, cost control, and investment.