Fill Out Your Annual Physical Examination Template
Fill Out Your Annual Physical Examination Template
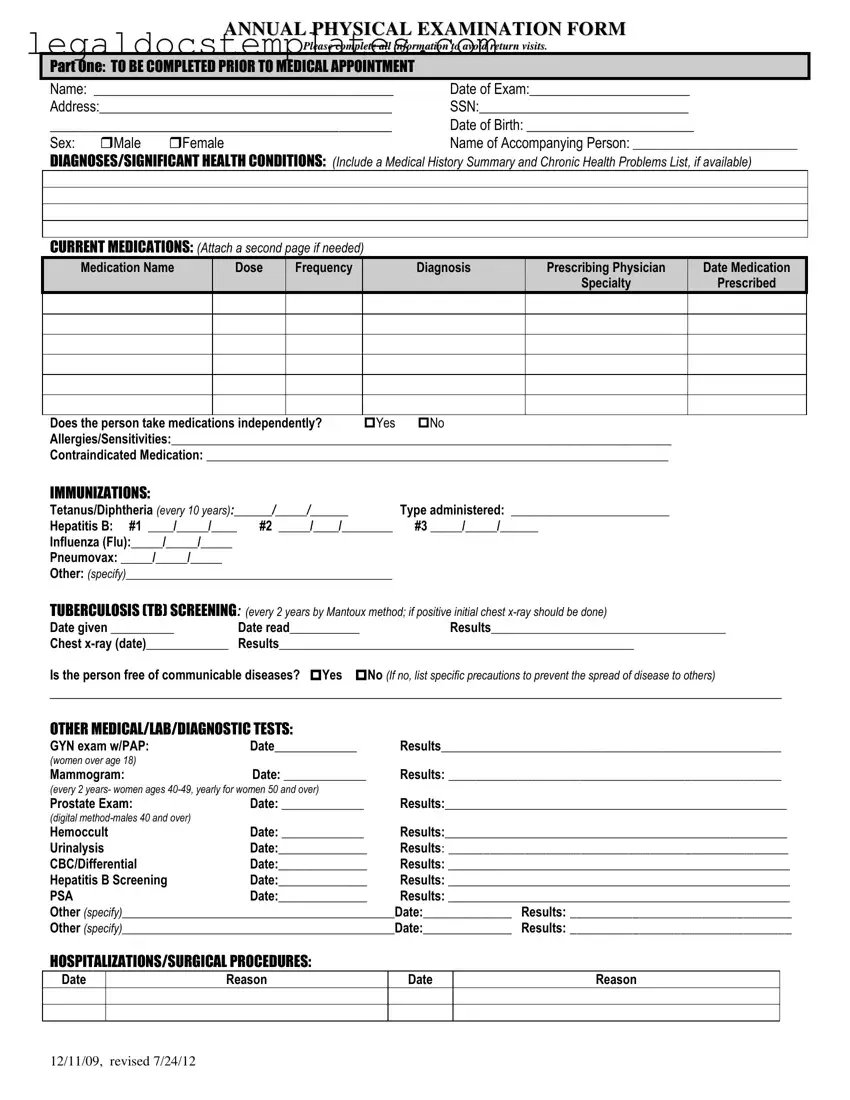
The Annual Physical Examination form serves as a comprehensive document designed to capture a wide range of health information, ensuring that individuals receive a detailed overview of their current physical condition. This multifaceted form requires input prior to a medical appointment, asking for personal details including name, date of birth, Social Security Number (SSN), and contact information. Moreover, it delves into a patient's medical history, chronic conditions, current medications—where details such as medication name, dosage, frequency, prescribing physician, and the reason for prescription need to be accurately filled. The form also covers a broad spectrum of vaccinations and screenings, such as for Tetanus/Diphtheria, Hepatitis B, Influenza, Pneumovax, and tuberculosis, alongside other essential medical, lab, and diagnostic tests ranging from urinalysis to mammograms and prostate exams depending on the patient’s sex and age. Hospitalization history, surgical procedures, and a general physical examination encompassing an evaluation of various systems from cardiovascular to musculoskeletal are integral parts as well. Additionally, it prompts for information on communicable diseases, potential activity limitations, use of adaptive equipment, and any changes in health status. The form also advise on health maintenance recommendations, including exercise, hygiene, and diet, while ensuring emergency information is up-to-date. The closure of the document calls for physicians’ observations on whether a detailed specialist evaluation is necessary, further imprinting its significance in guiding both patients and healthcare providers towards a proactive approach in maintaining and improving the individual's health.

ANNUAL PHYSICAL EXAMINATION FORM
Please complete all information to avoid return visits.
PART ONE: TO BE COMPLETED PRIOR TO MEDICAL APPOINTMENT
Name: ___________________________________________ |
Date of Exam:_______________________ |
Address:__________________________________________ |
SSN:______________________________ |
_____________________________________________ |
Date of Birth: ________________________ |
||
Sex: |
Male |
Female |
Name of Accompanying Person: __________________________ |
DIAGNOSES/SIGNIFICANT HEALTH CONDITIONS: (Include a Medical History Summary and Chronic Health Problems List, if available)
CURRENT MEDICATIONS: (Attach a second page if needed)
Medication Name |
Dose |
Frequency |
Diagnosis |
Prescribing Physician |
Date Medication |
|
|
|
|
Specialty |
Prescribed |
Does the person take medications independently? |
Yes |
No |
Allergies/Sensitivities:_______________________________________________________________________________ |
||
Contraindicated Medication: _________________________________________________________________________
IMMUNIZATIONS:
Tetanus/Diphtheria (every 10 years):______/_____/______ |
Type administered: _________________________ |
|
Hepatitis B: #1 ____/_____/____ |
#2 _____/____/________ |
#3 _____/_____/______ |
Influenza (Flu):_____/_____/_____ |
|
|
Pneumovax: _____/_____/_____ |
|
|
Other: (specify)__________________________________________ |
|
|
TUBERCULOSIS (TB) SCREENING: (every 2 years by Mantoux method; if positive initial chest |
||
Date given __________ |
Date read___________ |
Results_____________________________________ |
Chest |
Results________________________________________________________ |
|
Is the person free of communicable diseases? Yes No (If no, list specific precautions to prevent the spread of disease to others)
_________________________________________________________________________________________________________
OTHER MEDICAL/LAB/DIAGNOSTIC TESTS:
GYN exam w/PAP: |
Date_____________ |
Results_________________________________________________ |
(women over age 18) |
|
|
Mammogram: |
Date: _____________ |
Results: ________________________________________________ |
(every 2 years- women ages
Prostate Exam: |
Date: _____________ |
Results:______________________________________________________ |
|
(digital |
|
|
|
Hemoccult |
Date: _____________ |
Results:______________________________________________________ |
|
Urinalysis |
Date:______________ |
Results: _________________________________________________ |
|
CBC/Differential |
Date:______________ |
Results: ______________________________________________________ |
|
Hepatitis B Screening |
Date:______________ |
Results: ______________________________________________________ |
|
PSA |
Date:______________ |
Results: ______________________________________________________ |
|
Other (specify)___________________________________________Date:______________ |
Results: ________________________________ |
||
Other (specify)___________________________________________Date:______________ |
Results: ________________________________ |
||
HOSPITALIZATIONS/SURGICAL PROCEDURES:
Date
Reason
Date
Reason
12/11/09, revised 7/24/12
PART TWO: GENERAL PHYSICAL EXAMINATION
|
|
|
|
|
Please complete all information to avoid return visits. |
|
|
|
|
|
Blood Pressure:______ /_______ Pulse:_________ |
Respirations:_________ Temp:_________ Height:_________ |
Weight:_________ |
||||
|
|
EVALUATION OF SYSTEMS |
|
|
|
|
||
|
|
|
|
|
|
|
||
|
|
System Name |
|
Normal Findings? |
Comments/Description |
|
||
|
|
Eyes |
|
Yes |
No |
|
|
|
|
|
Ears |
|
Yes |
No |
|
|
|
|
|
Nose |
|
Yes |
No |
|
|
|
|
|
Mouth/Throat |
|
Yes |
No |
|
|
|
|
|
Head/Face/Neck |
|
Yes |
No |
|
|
|
|
|
Breasts |
|
Yes |
No |
|
|
|
|
|
Lungs |
|
Yes |
No |
|
|
|
|
|
Cardiovascular |
|
Yes |
No |
|
|
|
|
|
Extremities |
|
Yes |
No |
|
|
|
|
|
Abdomen |
|
Yes |
No |
|
|
|
|
|
Gastrointestinal |
|
Yes |
No |
|
|
|
|
|
Musculoskeletal |
|
Yes |
No |
|
|
|
|
|
Integumentary |
|
Yes |
No |
|
|
|
|
|
Renal/Urinary |
|
Yes |
No |
|
|
|
|
|
Reproductive |
|
Yes |
No |
|
|
|
|
|
Lymphatic |
|
Yes |
No |
|
|
|
|
|
Endocrine |
|
Yes |
No |
|
|
|
|
|
Nervous System |
|
Yes |
No |
|
|
|
|
|
VISION SCREENING |
|
Yes |
No |
Is further evaluation recommended by specialist? |
Yes |
No |
|
|
HEARING SCREENING |
|
Yes |
No |
Is further evaluation recommended by specialist? |
Yes |
No |
|
|
ADDITIONAL COMMENTS: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Medical history summary reviewed? |
Yes |
No |
|
|
||
Medication added, changed, or deleted: (from this appointment)__________________________________________________________
Special medication considerations or side effects: ________________________________________________________________
Recommendations for health maintenance: (include need for lab work at regular intervals, treatments, therapies, exercise, hygiene, weight control, etc.)
___________________________________________________________________________________________________________
Recommendations for manual breast exam or manual testicular exam: (include who will perform and frequency)____________________
___________________________________________________________________________________________________________
Recommended diet and special instructions: ____________________________________________________________________
Information pertinent to diagnosis and treatment in case of emergency:
___________________________________________________________________________________________________________
Limitations or restrictions for activities (including work day, lifting, standing, and bending): No Yes (specify)
___________________________________________________________________________________________________________ |
|||
Does this person use adaptive equipment? |
No |
Yes (specify):________________________________________________ |
|
Change in health status from previous year? No |
Yes (specify):_________________________________________________ |
||
This individual is recommended for ICF/ID level of care? (see attached explanation) Yes |
No |
||
Specialty consults recommended? No |
Yes (specify):_________________________________________________________ |
||
Seizure Disorder present? No Yes (specify type):__________________________________ Date of Last Seizure: ______________ |
|||
________________________________ |
_______________________________ |
_________________ |
|
Name of Physician (please print) |
Physician’s Signature |
|
Date |
Physician Address: _____________________________________________ |
Physician Phone Number: ____________________________ |
||
12/11/09, revised 7/24/12
| Fact | Description |
|---|---|
| Comprehensive Information Required | The form necessitates detailed personal and medical information, including medical history, current medications, allergies, immunizations, and results from various medical tests. |
| Regular Health Screenings | It emphasizes the importance of regular screenings such as TB, mammograms, prostate exams, and vaccinations to monitor and maintain health. |
| Update on Health Status | Patients are asked to report any change in their health status from the previous year, ensuring the form serves as a dynamic health record that reflects current conditions. |
| Emergency and Care Instructions | Provides space for instructions pertinent to diagnosis and treatment in emergencies, as well as recommendations for health maintenance, dietary instructions, and activity limitations or restrictions. |
Successfully completing the Annual Physical Examination form requires attention to detail and thoroughness to ensure accurate health records. This process is critical for maintaining updated medical information, which can significantly impact patient care and treatment plans. The following steps are designed to assist individuals or their caregivers in accurately filling out the form without the necessity of a return visit to complete or correct information.
Once the Annual Physical Examination form is fully completed with the patient's health information and the physician's assessment, it serves as a crucial part of the patient’s medical record. Ensuring accuracy and completeness can facilitate better healthcare outcomes and informed decisions regarding the patient's treatment and care plan.
The Annual Physical Examination Form is designed to ensure a comprehensive review of an individual's health status over the past year. By collecting detailed medical information, including diagnoses, current medications, immunization records, screening results, and hospitalization history, healthcare providers can deliver personalized care, prevent health issues, and manage ongoing conditions effectively.
Parts of the form are completed by different individuals to gather accurate and thorough information. Part One should be filled out by the patient, or an accompanying person if necessary, before the medical appointment to record personal and medical history. Part Two is for the healthcare provider to complete during the examination, documenting clinical findings and recommendations.
Providing detailed information about your current medications and allergies helps your healthcare provider to understand your treatment plan, avoid prescribing contraindicated medications, and prevent adverse drug interactions. This ensures your treatment plan is safe and effective for your specific health needs.
If you have more medications or health conditions than the space provided, you are encouraged to attach a second page with the additional information. This ensures your healthcare provider has a complete understanding of your health status and can make informed care decisions.
If your health status has changed, it's imperative to specify the type of change in the provided section. Whether it's a new diagnosis, a resolved condition, or a change in medication, these details help your healthcare provider assess your current health and update your care plan accordingly.
For individuals with seizure disorders, detailing the type of seizure, the date of the last seizure, and any medications prescribed for management is crucial. This information assists healthcare providers in monitoring the condition effectively and making any necessary adjustments to treatment plans or precautions to ensure patient safety.
One common mistake people make when filling out an Annual Physical Examination form is not providing complete information. This form requires precise details, such as social security numbers, addresses, and a comprehensive medical history, including chronic health problems. Neglecting to fill out these sections thoroughly may necessitate additional appointments, causing inconvenience and delays in receiving care.
Another error involves the section on current medications. Many individuals forget to attach a second page when the space provided is not sufficient, leading to incomplete medication documentation. This oversight can seriously impede medical professionals' ability to provide accurate and safe care, as they rely heavily on a patient's current medication list to make informed decisions about treatments and to avoid prescribing contraindicated medications.
Failure to accurately report allergies and sensitivities is also problematic. This part of the form is crucial for ensuring patient safety during the examination and any subsequent treatments. When allergies, especially to medications, are not clearly listed, healthcare providers may unintentionally expose patients to harmful substances. This mistake can result in adverse reactions, some of which could be severe.
Many people also neglect the sections pertaining to immunizations and tuberculosis (TB) screening. This information is vital for public health and individual care planning. Without accurate immunization records, healthcare providers might miss essential vaccines, putting the patient and those around them at risk for preventable diseases. Similarly, an incorrect or missing TB screening record can have serious consequences, considering the potential for spreading this disease.
Lastly, a frequent oversight is failing to update the form with changes in health status or new diagnoses since the last examination. This section is crucial for tracking a patient's health over time and ensuring they receive appropriate care for any new or worsening conditions. Without this information, physicians might not be fully aware of the patient's current health status, which can affect the quality of care and the ability to make informed decisions.
When attending a medical appointment, especially for an annual physical examination, several other forms and documents often accompany the main examination form. These documents ensure a comprehensive approach to health management, facilitating accurate diagnosis, personalized care plans, and effective follow-up. Here's a look at some of these crucial documents.
Together, the Annual Physical Examination form and its accompanying documents form a comprehensive toolkit for managing and monitoring health. They work in tandem to ensure that care providers have all the necessary information to offer personalized and effective healthcare, contribute to the continuity of care, and empower patients in their healthcare journeys.
The Annual Physical Examination form shares commonalities with a Pre-Operative Assessment form, mainly in gathering comprehensive patient health information ahead of medical procedures. Pre-Operative Assessments meticulously record a patient's medical history, allergies, current medications, and any past surgical procedures, mirroring the structured approach of the Annual Physical Examination form to compile a detailed medical profile. This ensures that healthcare providers are well-informed of any potential risks or necessary precautions before proceeding with surgery.
Similarly, the form aligns closely with a New Patient Intake form utilized by healthcare providers when a patient first registers with a new doctor or specialist. These forms typically require detailed personal information, medical history, and current health concerns, laying a foundation for patient care. The emphasis on collecting a broad spectrum of information from the onset facilitates a more tailored and effective healthcare approach, paralleling the comprehensive nature of the Annual Physical Examination form in establishing a patient's health baseline.
An Emergency Contact Information form is another document that bears resemblance in terms of capturing vital personal details for safety and precautionary measures. Although primarily focused on contact information, these forms often include brief medical history or specific health conditions that first responders or medical personnel need to be aware of in an emergency, much like the critical health data compiled in the Annual Physical Examination form.
The Medication Management Record, used by healthcare providers and patients alike, is designed to monitor and manage a patient's medication regimen. It requires detailed entries about the names, dosages, and frequencies of medications, akin to the medication section of the Annual Physical Examination form. Both documents play an essential role in avoiding drug interactions and ensuring the patient’s treatment plan is followed accurately.
The Immunization Record is a focused document that tracks a patient's history and updates of vaccinations, comparable to the immunization section included in the Annual Physical Examination form. It serves a crucial function in preventative health care, ensuring individuals are protected against various diseases and providing a clear record for schools, employment, or international travel. The inclusion of such information in the Annual Examination form highlights the importance of keeping immunization status current and accessible for overall health management.
Lastly, the Health Maintenance Checklist, which is used by healthcare providers to plan and track preventive services and screenings appropriate for patients based on their age, sex, and health status, shows similarities to the recommendations section of the Annual Physical Examination form. Both documents aim to identify and mitigate risk factors early on, encourage a proactive approach to health, and tailor preventive measures to the individual's specific health needs.
The Return to Work form, often required after an employee has been absent due to illness or injury, requires a comprehensive assessment of the individual’s ability to perform job duties safely. It may include sections on physical limitations, necessary accommodations, or restrictions, which are closely mirrored in the Annual Physical Examination form's sections on limitations or restrictions for activities and the use of adaptive equipment. This connection underscores the emphasis on evaluating and adapting to health conditions in both occupational and general health contexts.
When filling out the Annual Physical Examination form, it's crucial to ensure accuracy and completeness. Below are recommended dos and don'ts to guide you through this process.
Do:Many people have misconceptions about the Annual Physical Examination form. Understanding these can help ensure that the information provided is accurate and comprehensive, aiding in better health management. Here are the top ten misconceptions:
All sections must be filled out for everyone. Certain sections apply based on age, sex, and health conditions. For instance, a prostate exam is not relevant to females, just as a mammogram is not applicable to males.
The form is only for the doctor’s benefit. While it aids healthcare providers in assessing your health, it also ensures you receive tailored care and that nothing significant is overlooked.
Medication details are not crucial if you’re seeing a specialist. On the contrary, providing a complete list of medications, including dosages and frequencies, helps in managing your overall health and prevents drug interactions.
Immunization history is irrelevant for adults. Adults also need to keep their immunizations, like tetanus and influenza, up to date to prevent serious illnesses.
TB screening and chest x-rays are mandatory for all. These tests are typically required based on risk factors, exposure, or symptoms, not as a universal standard.
Past hospitalizations and surgeries have no impact on current health. Providing a complete history helps in understanding potential future health risks and managing existing conditions.
Diagnostic tests are optional. Tests such as urinalysis or CBC/differential are crucial for detecting issues that might not yet be symptomatic, ensuring early intervention.
A physical exam is just about checking vital signs. It’s a comprehensive review of bodily systems to detect any changes or abnormalities, even when you feel healthy.
Only new health information needs to be reported. Accurate current and past health information provides a full picture, helping to monitor changes or progress in health conditions.
You can only complete the form at the doctor’s office. Reviewing and starting the form beforehand can save time and ensure you don’t forget important information during your visit.
Understanding these misconceptions helps in preparing for your Annual Physical Examination. Providing detailed and accurate information facilitates better healthcare support, tailored to your personal health needs.
When it comes to your health, the Annual Physical Examination form plays a crucial role in ensuring that all your medical information is up-to-date and thoroughly documented. Here are seven key takeaways to consider when filling out and using this form:
By paying close attention to these aspects, you can ensure that your Annual Physical Examination form is an accurate and comprehensive snapshot of your health, which is instrumental in receiving the best possible care.
IRS E-file Signature Authorization - Form 8879 also ensures that electronic filings comply with IRS regulations, making it a critical document for tax compliance.
Different Types of Background Checks - The requirement for detailed contact information for references ensures that Cracker Barrel can conduct thorough and accurate employment verifications.
Short Term Disability California - It's a key document for individuals undergoing treatments or surgeries that prevent them from working.