Fill Out Your Ada Dental Claim Template
Fill Out Your Ada Dental Claim Template
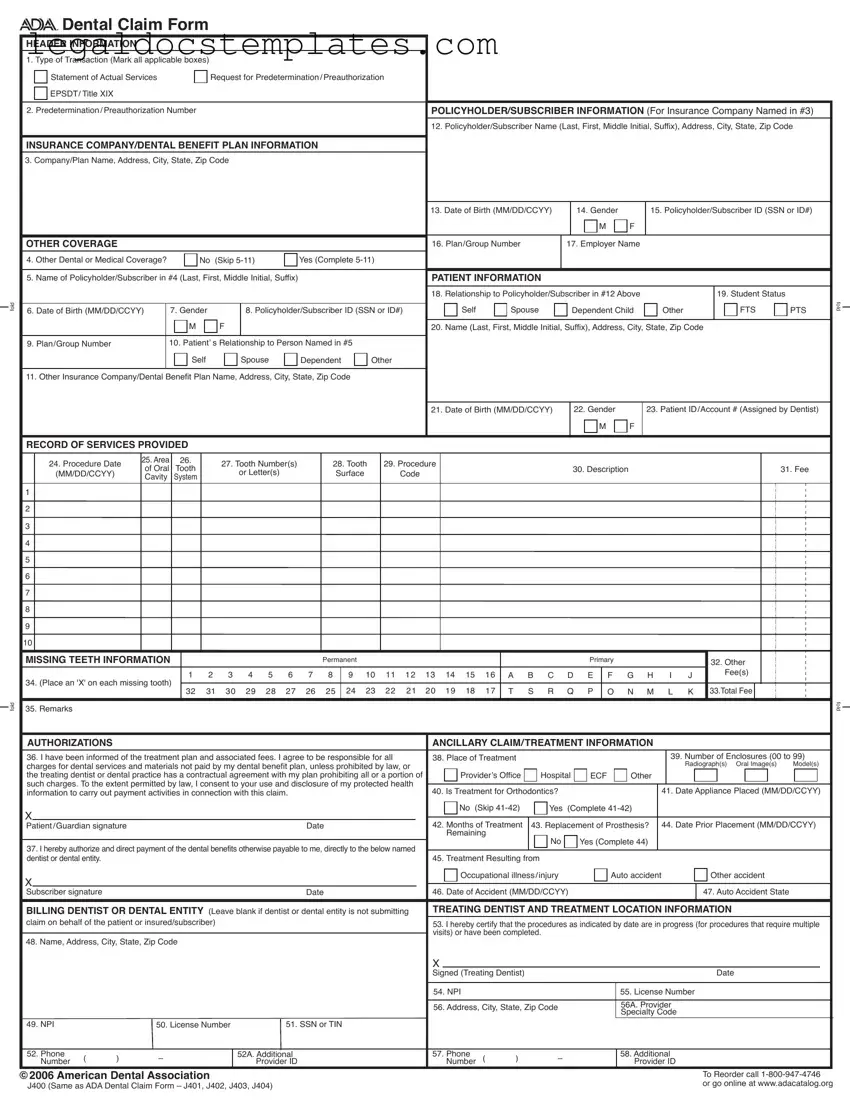
Navigating the complexities of dental insurance claims is crucial for both dental professionals and patients, ensuring that necessary treatments are covered and reimbursed efficiently. Central to this process is the ADA Dental Claim Form, a standardized document widely utilized across the United States by dental offices to submit claims to insurance companies. This form captures detailed information across several sections including header information, policyholder/subscriber and insurance company/dental benefit plan information, other coverage details, patient information, a record of services provided, and details about missing teeth, among other crucial data points. Also incorporated are sections for authorizations, ancillary claim/treatment information, and details specific to the billing and treating dentist or dental entity. The form is designed for clarity, with specific instructions on how to fold and submit it, ensuring that the claim reaches the insurance company in a format that facilitates prompt processing. Additionally, it incorporates modern requirements such as the National Provider Identifier (NPI) for the submitting dentist or dental entity, acknowledging the evolving landscape of healthcare and insurance information management. The ADA provides comprehensive guidelines on completing the claim form, geared towards streamlining the submission process and expediting the reimbursement of dental claims.
fold
fold



 Dental Claim Form
Dental Claim Form
HEADER INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
1. Type of Transaction (Mark all applicable boxes) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Statement of Actual Services |
|
|
Request for Predetermination/Preauthorization |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
EPSDT/ Title XIX |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. Predetermination/Preauthorization Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
POLICYHOLDER/SUBSCRIBER INFORMATION (For Insurance Company Named in #3) |
|
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12. Policyholder/Subscriber Name (Last, First, Middle Initial, Suffix), Address, City, State, Zip Code |
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
INSURANCE COMPANY/DENTAL BENEFIT PLAN INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
3. Company/Plan Name, Address, City, State, Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13. Date of Birth (MM/DD/CCYY) |
|
|
14. Gender |
|
|
15. Policyholder/Subscriber ID (SSN or ID#) |
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
OTHER COVERAGE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
16. Plan/Group Number |
|
|
17. Employer Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
4. Other Dental or Medical Coverage? |
|
|
No (Skip |
|
|
Yes (Complete |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
5. Name of Policyholder/Subscriber in #4 (Last, First, Middle Initial, Suffix) |
|
|
|
|
|
|
|
PATIENT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
18. Relationship to Policyholder/Subscriber in #12 Above |
|
|
|
|
|
|
|
19. Student Status |
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Self |
|
Spouse |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FTS |
PTS |
fold |
|||||||||
6. Date of Birth (MM/DD/CCYY) |
|
7. Gender |
|
|
|
8. Policyholder/Subscriber ID (SSN or ID#) |
|
|
|
Dependent Child |
Other |
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
M |
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
20. Name (Last, First, Middle Initial, Suffix), Address, City, State, Zip Code |
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
9. Plan/Group Number |
|
|
10. Patient’ s Relationship to Person Named in #5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
Self |
|
|
|
Spouse |
|
Dependent |
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
11. Other Insurance Company/Dental Benefit Plan Name, Address, City, State, Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
21. Date of Birth (MM/DD/CCYY) |
|
|
22. Gender |
|
|
23. Patient ID/Account # (Assigned by Dentist) |
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
RECORD OF SERVICES PROVIDED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
24. Procedure Date |
25. Area |
26. |
|
27. Tooth Number(s) |
|
|
28. Tooth |
29. Procedure |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
of Oral |
Tooth |
|
|
|
|
|
|
|
|
|
30. Description |
|
|
|
|
|
|
|
|
|
|
|
31. Fee |
|
||||||||||||||||||||||||||||
|
(MM/DD/CCYY) |
|
|
|
|
or Letter(s) |
|
|
|
Surface |
Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
Cavity |
System |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
MISSING TEETH INFORMATION |
|
|
|
|
|
|
|
|
|
|
Permanent |
|
|
|
|
|
|
|
|
|
|
Primary |
|
|
|
|
|
|
|
|
|
32. Other |
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
8 |
|
9 10 11 12 13 14 15 16 |
A B C D E |
F G H |
|
I |
J |
|
|
|
|
Fee(s) |
|
|
|
|
|
|
|
|||||||||||||||||||
34. (Place an 'X' on each missing tooth) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
32 |
31 |
30 |
29 |
28 |
27 |
26 |
|
25 |
|
24 23 |
22 21 |
|
20 19 18 |
17 |
T |
S R |
Q |
P |
O |
N M |
|
L |
K 33.Total Fee |
|
|
|
|
|
|
|
||||||||||||||||
35. Remarks |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
fold |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
AUTHORIZATIONS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ANCILLARY CLAIM/TREATMENT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
36. I have been informed of the treatment plan and associated fees. I agree to be responsible for all |
38. Place of Treatment |
|
|
|
|
|
|
|
|
|
|
|
|
39. Number of Enclosures (00 to 99) |
|
||||||||||||||||||||||||||||||||||||||
charges for dental services and materials not paid by my dental benefit plan, unless prohibited by law, or |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Radiograph(s) Oral Image(s) |
Model(s) |
|
|||||||||||||||||||||||||||||||||
the treating dentist or dental practice has a contractual agreement with my plan prohibiting all or a portion of |
|
Provider’s Office |
Hospital |
ECF |
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
such charges. To the extent permitted by law, I consent to your use and disclosure of my protected health |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
information to carry out payment activities in connection with this claim. |
|
|
|
|
|
|
|
40. Is Treatment for Orthodontics? |
|
|
|
|
|
|
|
|
|
41. Date Appliance Placed (MM/DD/CCYY) |
|
||||||||||||||||||||||||||||||||||
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
No (Skip |
Yes |
(Complete |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient/Guardian signature |
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
42. Months of Treatment |
43. Replacement of Prosthesis? |
|
44. Date Prior Placement (MM/DD/CCYY) |
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Remaining |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
37. I hereby authorize and direct payment of the dental benefits otherwise payable to me, directly to the below named |
|
|
|
|
No |
|
|
Yes (Complete 44) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
dentist or dental entity. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
45. Treatment Resulting from |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Occupational illness/injury |
|
|
|
Auto accident |
|
|
|
|
|
Other accident |
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Subscriber signature |
|
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
46. Date of Accident (MM/DD/CCYY) |
|
|
|
|
|
|
|
|
|
|
47. Auto Accident State |
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
BILLING DENTIST OR DENTAL ENTITY (Leave blank if dentist or dental entity is not submitting |
TREATING DENTIST AND TREATMENT LOCATION INFORMATION |
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||
claim on behalf of the patient or insured/subscriber) |
|
|
|
|
|
|
|
|
|
|
|
|
|
53. I hereby certify that the procedures as indicated by date are in progress (for procedures that require multiple |
|
||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
visits) or have been completed. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
48. Name, Address, City, State, Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signed (Treating Dentist) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
54. NPI |
|
|
|
|
|
|
|
|
|
55. License Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
56. Address, City, State, Zip Code |
|
|
|
|
|
56A. Provider |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Specialty Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
49. NPI |
|
|
50. License Number |
|
|
|
51. SSN or TIN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
52. Phone |
( |
) |
– |
|
|
|
|
|
52A. Additional |
|
|
|
|
|
|
|
57. Phone |
( |
) |
– |
|
|
|
|
|
58. Additional |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
Number |
|
|
|
|
|
|
|
Provider ID |
|
|
|
|
|
|
|
|
Number |
|
|
|
|
|
Provider ID |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
©2006 American Dental Association |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
To Reorder call |
|
||||||||||||||||||||
J400 (Same as ADA Dental Claim Form – J401, J402, J403, J404) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
or go online at www.adacatalog.org |
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
Comprehensive completion instructions for the ADA Dental Claim Form are found in Section 4 of the ADA Publication titled
GENERAL INSTRUCTIONS
A. The form is designed so that the name and address (Item 3) of the
B. In the
assignment of a claim or control number.
|
C. All Items in the form must be completed unless it is noted on the form or in the following instructions that completion is not required. |
|
|
D. When a name and address field is required, the full name of an individual or a full business name, address and zip code must be entered. |
|
|
E. All dates must include the |
|
|
F. If the number of procedures reported exceeds the number of lines available on one claim form, the remaining procedures must be |
|
listed on a separate, fully completed claim form. |
|
COORDINATION OF BENEFITS (COB)
When a claim is being submitted to the secondary payer, complete the form in its entirety and attach the primary payer’s Explanation of Benefits (EOB) showing the amount paid by the primary payer. You may indicate the amount the primary carrier paid in the “Remarks” field (Item # 35).
NATIONAL PROVIDER IDENTIFIER (NPI)
49 and 54 NPI (National Provider Indentifier): This is an identifier assigned by the Federal government to all providers considered to be HIPAA covered entities. Dentists who are not covered entities may elect to obtain an NPI at their discretion, or may be enumerated if required by a participating provider agreement with a
ADDITIONAL PROVIDER IDENTIFIER
52A and 58 Additional Provider ID: This is an identifier assigned to the billing dentist or dental entity other than a Social Security Number (SSN) or Tax Identification Number (TIN). It is not the provider’s NPI. The additional identifier is sometimes referred to as a Legacy Identifier (LID). LIDs may not be unique as they are assigned by different entities (e.g.,
PROVIDER SPECIALTY CODES
56A Provider Specialty Code: Enter the code that indicates the type of dental professional who delivered the treatment. Available codes describing treating dentists are listed below. The general code listed as ‘Dentist’ may be used instead of any other dental practitioner code.
Category / Description Code |
Code |
|
|
Dentist |
|
A dentist is a person qualified by a doctorate in dental surgery (D.D.S) |
122300000X |
or dental medicine (D.M.D.) licensed by the state to practice dentistry, |
|
and practicing within the scope of that license. |
|
|
|
General Practice |
1223G0001X |
Dental Specialty (see following list) |
Various |
Dental Public Health |
1223D0001X |
Endodontics |
1223E0200X |
Orthodontics |
1223X0400X |
Pediatric Dentistry |
1223P0221X |
Periodontics |
1223P0300X |
Prosthodontics |
1223P0700X |
Oral & Maxillofacial Pathology |
1223P0106X |
Oral & Maxillofacial Radiology |
1223D0008X |
Oral & Maxillofacial Surgery |
1223S0112X |
Dental provider taxonomy codes listed above are a subset of the full code set that is posted at:
Should there be any updates to ADA Dental Claim Form completion instructions, the updates will be posted on the ADA’s web site at:
www.ada.org/goto/dentalcode
| Fact | Description |
|---|---|
| Transaction Types | Indicates whether the form is for actual services provided, a request for predetermination/preauthorization, or related to EPSDT/Title XIX. |
| Policyholder Information | Includes the policyholder's name, address, city, state, and zip code, necessary for identifying the insured or subscriber for the insurance company. |
| Insurance Company Information | List the dental plan or insurance company's name, address, city, state, and zip code to which the claim is sent. |
| Other Coverage | Details if there is any other dental or medical coverage and requires completion of additional policyholder information if applicable. |
| Patient Information | Covers the patient's name, relationship to the policyholder, student status, address, date of birth, and gender. |
| Record of Services | Details the services provided, including dates, procedure codes, tooth numbers, and fees. |
| Missing Teeth Information | Includes a section to indicate any teeth that are missing prior to the current treatment. |
| Ancillary Claim/Treatment Information | Contains authorizations, treatment location, number of enclosures, and if the treatment is for orthodontics or a replacement of prosthesis. |
| Provider IDs and Specialty Codes | Includes National Provider Identifier (NPI), Tax Identification Number (TIN), and specialty codes to properly identify the treating dentist or dental entity. |
Filling out the ADA Dental Claim form accurately is crucial for timely and correct processing of dental insurance claims either for reimbursement or predetermination of benefits. This process involves providing comprehensive patient information, details about the dental service provided, and information on the billing and treating dentist. The steps outlined below should help in completing this form meticulously.
Once all sections of the ADA Dental Claim Form are completed, review the entire document for accuracy and completeness. Ensure that the form is folded according to the fold marks for mailing in a standard #10 window envelope. Submit the form to the designated insurance company or dental benefit plan for processing. Accurate and thorough completion helps expedite claim processing, ensuring timely reimbursement and application of benefits.
The ADA Dental Claim Form is a critical document in the dental industry, serving multiple purposes. Primarily, it is used to request reimbursement from a dental insurance company for dental services provided to a patient. The form facilitates the submission of dental claims by outlining the details of the services rendered, including procedures performed, dates, and associated costs. It can also be used for requesting predeterminations or preauthorizations for dental services, to verify whether the proposed treatments are covered by the patient's dental plan and to what extent. Furthermore, the form helps in submitting claims for actual services provided, ensuring that healthcare providers receive payment for their services in a timely manner.
To ensure accurate processing of a dental claim, the ADA Dental Claim Form must be filled out comprehensively and accurately, following specific steps outlined by the American Dental Association (ADA).
It's important that every field on the form is completed unless noted otherwise in the instructions to avoid any delays in claim processing.
If a patient has additional dental or medical insurance, it is crucial to complete sections 4 through 11 of the ADA Dental Claim Form. This process, known as Coordination of Benefits (COB), ensures that all insurance policies contribute to the patient’s dental expenses in an orderly manner. One must indicate whether the other coverage is dental or medical and provide details of the secondary policy, including the policyholder's name, date of birth, gender, and identification number. For the secondary insurance claim submission, attach the primary insurer’s Explanation of Benefits (EOB) that shows what was covered and the amount paid, and note this payment in the “Remarks” section (Item #35) of the form for the secondary insurer's reference.
In the treatment section of the ADA Dental Claim Form, detailed information about the procedures performed must be provided. This includes the date of each procedure, a description of the work done, tooth numbers or areas treated, procedure codes, and the fees charged for each service. Accurate and complete entries here are essential for the insurance company to evaluate and process the claim efficiently. Additionally, if treatments are part of an ongoing series, indicate the procedures that are in progress. Any missing teeth should also be marked in the provided chart, as this can affect coverage for certain procedures.
The National Provider Identifier (NPI) is a unique identification number for covered healthcare providers, mandated by the Health Insurance Portability and Accountability Act (HIPAA) of 1996. On the ADA Dental Claim Form, the treating dentist or dental entity's NPI is entered in fields 49 and 54. This identifier helps in streamlining the claim process by uniquely identifying the provider. If applicable, an Additional Provider Identifier (API) can also be included in fields 52A and 58. The API is used for identification purposes by some insurance plans and may be required in addition to the NPI, based on specific payer requirements or for dentists participating in certain networks.
Yes, the ADA Dental Claim Form can be submitted electronically to most dental insurance companies, which is encouraged for efficiency and environmental reasons. Electronic submission, also known as electronic data interchange (EDI), allows for quicker processing of claims and reduces the potential for errors associated with manual data entry. Dental practices need to use compliant dental practice management software that can produce and send claims in the correct electronic format. Providers should check with each insurance company for specific submission guidelines and requirements to ensure compliance and to facilitate prompt and accurate payment.
Filling out the ADA Dental Claim Form can sometimes be a bit like navigating a maze, especially if you're not familiar with the process. Mistakes can be easy to make but can lead to delays or denials of claims. Here are ten common pitfalls that people often encounter when completing this form.
One frequently seen error involves the Type of Transaction section. It's important to thoroughly mark all applicable boxes that describe the nature of the claim being submitted. Overlooking this step can cause confusion about what is being requested, whether it's for actual services rendered or a request for predetermination/preauthorization.
Another common mistake is not providing complete policyholder/subscriber information. Item 12, which requires the policyholder's name, address, city, state, and zip code, is often filled out incorrectly or incompletely. Ensuring that this information is accurate and fully detailed is crucial, as it helps to identify the responsible party for insurance purposes.
Furthermore, misunderstanding the coverage section, particularly when it comes to Other Dental or Medical Coverage, leads to issues. If there is other coverage, sections 5-11 must be completed in full. Neglecting this can result in the claim being delayed or denied if the insurance company detects other applicable coverage after submission.
The patient's information, especially their relationship to the policyholder and their student status, is often filled out incorrectly. Boxes 18 and 19 are designed to gather this information, and accuracy here is key to establishing who the patient is in relation to the insured and their coverage eligibility, especially for dependents.
Misidentifying the treating dentist and treatment location, areas covered in sections 48-58, can also lead to claim setbacks. It's crucial to provide the correct identification and specialty codes for the provider, as this information helps ensure that the claim is processed promptly and accurately.
A common error takes place in the Record of Services Provided area, where specific details about the dental procedures need to be meticulously documented. Mistakes in coding or failing to list all relevant details, such as tooth numbers and procedure dates, can lead to claim rejections or unnecessary back-and-forth with insurance companies.
Many also stumble on accurately completing the Missing Teeth Information section. This area is essential for accurate claims related to treatments involving tooth replacement and must be filled out with attention to which teeth are missing and since when.
The Authorizations section is another critical component often overlooked or improperly completed. This section requires signatures to authorize treatment and claim submission. Forgetting to sign or dating incorrectly can invalidate a claim.
Inaccuracies in reporting the Treatment Resulting from section, which involves specifying the cause of dental conditions—like accidents or occupational hazards—can misdirect the processing of claims, affecting coverage eligibility.
Lastly, a frequent oversight occurs with the National Provider Identifier (NPI) and Additional Provider Identifier. These identifiers are unique to each provider and essential for claim processing. Confusing these numbers or entering them incorrectly can direct the claim to the wrong provider or delay its processing.
Avoiding these mistakes requires careful attention to detail and a thorough understanding of the claim submission process. By taking your time to double-check every section and ensuring all information is complete and correct, you can help streamline the claims process and avoid unnecessary delays or denials.
When processing dental claims, the ADA Dental Claim Form serves as the foundation for submitting dental treatment information to insurance companies. However, to ensure a seamless claims process and to enhance the likelihood of a successful reimbursement, it’s often necessary to accompany this primary document with additional forms and documents. Here, we outline five critical documents often used alongside the ADA Dental Claim Form, elucidating their purpose and the role they play in the claims process.
By compiling these documents alongside the ADA Dental Claim Form, dental practices can provide a comprehensive package that supports the claims made, ensuring that insurance companies have all the information necessary to process and approve claims efficiently. This not only streamlines the reimbursement process but also aids in managing patient expectations and contributes to the overall efficiency of the dental practice’s operations.
The ADA Dental Claim Form is quite similar to the Medical Claim Form used by healthcare providers to bill insurance companies for medical services provided. Both forms capture detailed information about the patient, insurance coverage, and the specific services rendered. They include sections for policyholder information, patient demographics, service provider details, and a breakdown of charges. The primary difference lies in the specific nature of services and codes reported—dental versus general medical.
Another document that resembles the ADA Dental Claim Form is the Prescription Drug Claim Form. This form is used by pharmacies to request reimbursement from insurance companies for medications dispensed to insured patients. Like the dental claim form, it collects information on the patient, prescriber, and insurance coverage, but instead focuses on the specific medications dispensed, their quantities, and associated costs.
The Vision Care Claim Form bears similarities to the ADA Dental Claim Form as well. Designed for optometrist and ophthalmologist offices, it details patient and insurance information, along with services provided, such as eye exams, glasses, or contact lens fittings. Both forms serve the purpose of detailing specialized healthcare services for insurance reimbursement, though they cater to different types of services (dental vs. vision care).
The Workers' Compensation Claim Form is used by employees to file for benefits due to a workplace injury or illness. While its primary function is to initiate a claim for workers' compensation benefits rather than direct billing to insurance, it similarly collects detailed information about the claimant, the employer, and the medical provider. The focus is on the nature of the injury or illness, treatments received, and work status, paralleling the data collection aspect of the ADA Dental Claim Form but for a different purpose.
The Health Insurance Claim Form (often known as the CMS-1500) is used by non-institutional providers to bill Medicare and other health insurance programs. Like the ADA Dental Claim Form, it collects detailed information about the patient, the provider, the insurance coverage, and the services provided, including detailed service codes and charges. Both forms are integral to the healthcare reimbursement process, though the CMS-1500 is broader in its application across various medical services.
The Patient Registration Form, commonly used in both medical and dental practices, gathers patient demographic and insurance information at the point of service. Although not a claim form per se, it captures many of the same initial data points as the ADA Dental Claim Form, such as patient name, contact information, insurance details, and relationship to the policyholder. This form is crucial for the backend billing processes, including the completion of claim forms.
The Durable Medical Equipment (DME) Claim Form is used to bill for rental or purchases of equipment intended for medical use at home, like wheelchairs or hospital beds. Similar to the ADA Dental Claim Form, it requires information about the patient, the prescriber/provider, and the insurance coverage. The main difference lies in the type of services and items billed, focusing on equipment rather than procedural services.
The Automobile Personal Injury Protection (PIP) Claim Form is used for billing auto insurance carriers for medical treatment following an auto accident. It shares similarities with the ADA Dental Claim Form in that it captures patient information, details of the insurance policy, and specifics of the medical services provided due to the accident. However, it is tailored to auto insurance and personal injury protection coverage specifics.
The Travel Insurance Claim Form is used by individuals to claim for medical services received or losses incurred while traveling. Though its primary purpose is broader, covering a range of benefits like trip cancellations and lost luggage, the sections related to medical services resemble those in the ADA Dental Claim Form. Both require detailed documentation of services received, costs, and insurance information, even though the contexts in which they are used differ significantly.
The Disability Insurance Claim Form, used to apply for benefits under a disability insurance policy, gathers comprehensive information about the claimant's medical condition, treatment history, and ability to work. While focused more on the disability aspect and less on detailed billing for specific services (like the ADA Dental Claim Form), it nonetheless collects extensive health and provider information to substantiate a claim for benefits based on health conditions that impact the claimant's life and work.
When filling out the ADA Dental Claim form, it's important to keep a few best practices in mind to ensure accurate and timely processing of your claim. Here's a helpful guide:
Do:When it comes to dealing with ADA Dental Claim forms, many people hold onto misconceptions that could interfere with the processing of their dental claims efficiently. Here's a list of the nine most common misconceptions and the truths behind them:
Clearing up these misconceptions ensures a smoother experience for patients, dental practices, and insurance companies alike, fostering efficient communication and reducing the chances of claim denial or delay.
Filling out the ADA Dental Claim Form correctly is crucial for a smooth claims process. Here are key takeaways to ensure accuracy and compliance:
By paying close attention to these guidelines, dental professionals and their administrative staff can help ensure that claims are processed efficiently and accurately, minimizing the need for re-submissions and reducing delays in payments.
Electrical Load Calculation - A vital step in obtaining building permits, as it verifies conformity with electrical safety standards.
Aoa Rental Application - By demanding a detailed employment history, the form indirectly assesses the applicant’s stability and reliability as a tenant.